
What is Retatrutide?
The evidence, potential benefits and remaining uncertainties.
The evidence, potential benefits and remaining uncertainties.
There is no denying the impact glucagon-like peptide-1 receptor agonists (GLP-1s or GLP-1RAs) have had on the treatment of obesity in recent years. These medications are commonly known as ‘fat loss jabs’ or ‘skinny jabs’, and every day there seems to be a story in the media documenting a celebrity’s dramatic weight loss from using these novel medications.
As with any innovation, earlier versions are inevitably superseded by later, more advanced editions that promise even greater benefits. GLP-1s are no exception. Since the first injectable weight loss pharmacotherapy began in 2014 with the approval of liraglutide 3.0 mg (Saxenda), injectable obesity treatments have progressed rapidly.
The latest step in this evolution is the much-anticipated first triple-agonist, retatrutide. Although currently in Phase 3 trials and not due for release to the public for at least a year or more, evidence suggests that it can produce unprecedented weight loss results. While the results so far are striking, it is important to understand that retatrutide is still in early-stage clinical development and the long-term safety profile remains unknown.
This article will provide an objective overview of the current evidence relating to the efficacy and safety of retatrutide and how it may be best used.
GLP-1s are a group of medications that mimic glucagon-like peptide 1, a natural hormone released after eating that helps to regulate appetite, blood sugar, and digestion. They work by slowing gastric emptying, reducing hunger signals in the brain, and enhancing insulin release while suppressing glucagon. This combination helps to lower blood glucose and reduce caloric intake, leading to a reduction in body mass. In the UK, there are several licensed GLP-1 medicines including:
While semaglutide is classed as a single-agonist because it contains only GLP-1, tirzepatide is known as a dual agonist because, in addition to GLP-1, it also contains glucose-dependent insulinotropic polypeptide (GIP).
Like GLP-1, GIP is a hormone released from the gut after eating, where it enhances insulin secretion and influences energy balance through receptors in the pancreas, adipose tissue, and the brain. Its standalone metabolic effects are relatively modest, but when combined with GLP-1, it makes the appetite-reducing effect considerably greater.
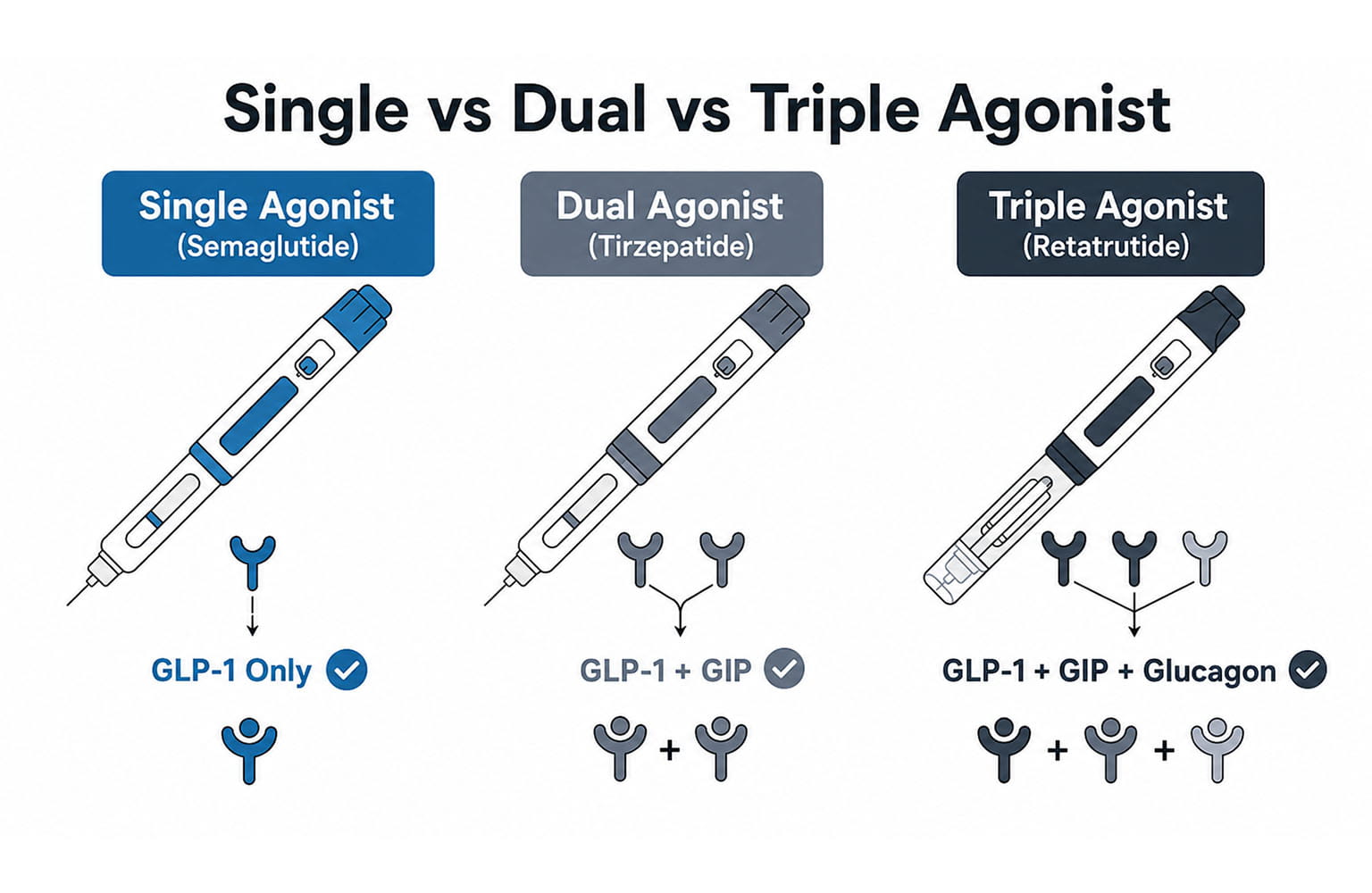
Retatrutide is known as a triple-agonist because, in addition to GLP-1 and GIP, it also contains the naturally occurring hormone, glucagon. Although most widely known for its ability to elevate blood glucose levels when they are low, glucagon also has fat-mobilising (lipolytic) effects, stimulating the breakdown of stored triglycerides into free fatty acids that can be used for energy.
In addition, it increases energy expenditure by activating hepatic and brown fat pathways and increases overall fat-burning potential. In short, the combination of GLP-1, GIP and glucagon produces a greater reduction in appetite accompanied by greater use of stored fat for energy and increased energy expenditure.
As impressive as the science sounds, does this combination actually result in greater weight loss than any single or dual agonist?
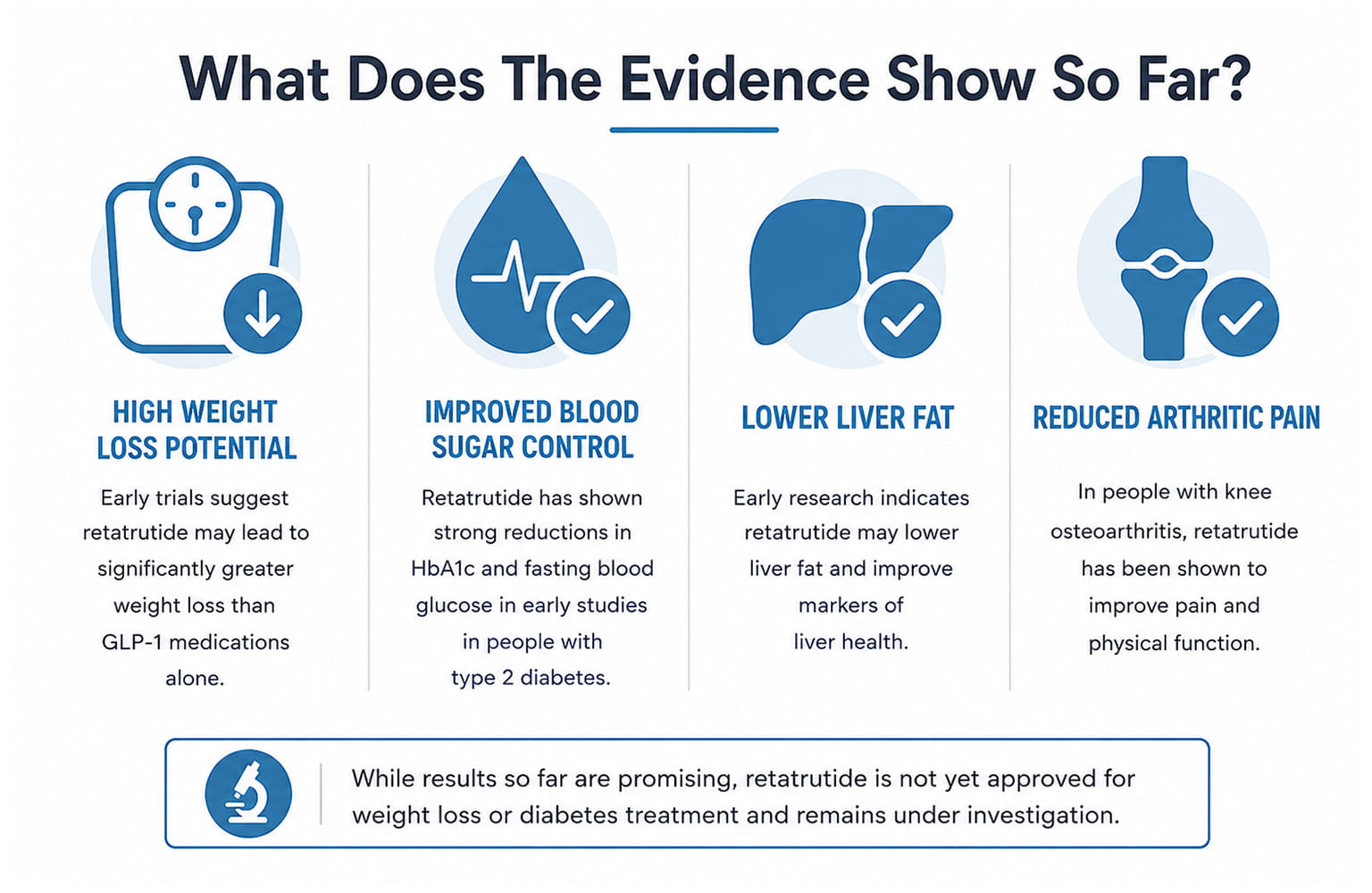
The current evidence suggests that it does. In a Phase 2 trial published in The New England Journal of Medicine, participants receiving the highest dose of retatrutide achieved up to 24.2% mean weight loss at 48 weeks. In some cases, this was comparable to bariatric surgery (1).
| Medication | Mechanism | Weight-loss range |
| Retatrutide | GLP‑1 + GIP + glucagon | ~24% at 48 weeks 29% (1,2,3) |
| Tirzepatide | GLP‑1 + GIP | ~20–22% at 72 weeks (4) |
| Semaglutide | GLP‑1 | ~13–15% at 68 weeks (5) |
| Liraglutide | GLP‑1 | ~5–8% at 1 year (6) |
To gain a fuller and more detailed understanding of the benefits and potential problems associated with retatrutide, it is important to look beyond the media headlines and hype, and examine a selection of the research that has been published so far.
Presented here are four studies that provide useful insight into our current understanding of retatrutide.
Jastreboff et al. (1) conducted a phase 2, double-blind, randomised, placebo-controlled trial in adults with BMI ≥30 or BMI 27–<30 and a weight-related condition. This is considered to be a landmark study because it was the first human trial to show the full clinical potential of a triple-agonist therapy.
Participants were assigned to a weekly retatrutide dose of 1 mg, 4 mg, 8 mg or 12 mg or a placebo for 48 weeks.
The results showed that at 48 weeks, the average weight loss was:
Results also showed:
The findings of Jastreboff et al. (1) concur with those of a study by Rosenstock and colleagues (7). This phase 2 trial involved 281 adults with type 2 diabetes and a BMI of 25–50, who were on lifestyle therapy with or without stable metformin.
Participants were randomised to receive once-weekly retatrutide (0.5–12 mg) or dulaglutide (1.5 mg) for 36 weeks.
The results showed:
A more recent study (8) expanded retatrutide’s potential beyond obesity and diabetes into liver disease. This randomised phase 2 trial assessed the effects of once-weekly retatrutide in adults with metabolic dysfunction–associated fatty liver disease.
The findings demonstrated that liver fat fell sharply at 24 weeks in a dose-dependent manner, dropping by:
This was compared with no change for the placebo.
Normal liver fat levels were reached by up to 86% of participants using retatrutide versus 0% on placebo.
These reductions closely tracked improvements in body weight, abdominal fat, and metabolic markers linked to better insulin sensitivity and lipid metabolism.
By week 48, body weight reductions of 22.8% and 24.2% were achieved with doses of 8 and 12 mg, respectively.
An unexpected effect of retatrutide is a reduction in arthritic pain.
The latest Phase 3 TRIUMPH-4 data (9), although not yet peer-reviewed, show that retatrutide produces meaningful reductions in knee osteoarthritis pain in adults who are obese or overweight.
At 68 weeks, the 9 mg and 12 mg doses reduced pain scores by approximately 4.5 points, with a high proportion of participants achieving complete pain resolution.
Improvements also extended to physical function and stiffness, indicating broad symptomatic benefit.
These effects occurred alongside substantial weight loss of up to 28%.
While this reduces joint loading, a reduction in inflammatory markers indicates an additional anti-inflammatory effect.
The authors suggest these findings highlight retatrutide’s potential as a promising therapy for obesity-associated knee OA, offering pain relief, functional gains, and metabolic improvements in a population with limited effective options.
As promising and as remarkable as these preliminary results appear, it is important to understand that there are still significant gaps in our current knowledge of retatrutide.
There are a number of issues seen across the studies which contribute to our limited understanding. These include:
As with many medications, retatrutide has been associated with a number of side effects.
Across the literature, these tend to be cited as being mild-to-moderate, similar to other GLP-1 medications and mainly gastrointestinal in nature. Typically, these include nausea, diarrhoea, vomiting, constipation, decreased appetite and early fullness (1,7,8). Fatigue, headache, and dizziness are also reported (15).
To fully appreciate the potential adverse events of retatrutide, we need to delve a little deeper into the data.
This is made easier by the recent publication of a comprehensive review of retatrutide’s safety profile based on Phase 1, Phase 2, and Phase 3 TRIUMPH-4 clinical trial data (15). This highlights several important concerns:
Dysesthesia is a new safety signal identified in the Phase 3 trials. It refers to an unpleasant abnormal sensation that occurs either spontaneously or in response to a normally non-painful stimulus. It is not known if it resolves with continued treatment, whether it is associated with specific neurological findings on examination, and whether it affects treatment adherence in real-world settings.
While the clinical trials show a reduction in blood pressure and unhealthy blood fats, retatrutide is associated with a modest increase in resting heart rate of approximately 2–4 beats per minute. The long-term effects and relevance of this increase are not currently known.
GLP-1 drugs include a precautionary warning about a rare thyroid cancer (medullary thyroid carcinoma). This is because rats given these medicines developed C-cell tumours, though this may not apply to humans since our thyroid C cells have far fewer GLP-1 receptors. In retatrutide’s Phase 2 studies, researchers monitored calcitonin—a marker of C-cell activity. Although no increases were observed, it is important to note that the trials were too small and too short to rule out a long-term thyroid cancer risk.
Rapid weight loss from any cause, including weight-loss medication, is associated with an increased risk of gallbladder problems. A small number of gallbladder-related adverse events have been reported in the active treatment groups in the studies, which are consistent with the known association between significant weight loss and gallstone formation. Retatrutide’s more potent weight loss effect may heighten this risk.
Reactions at the injection site, including redness, swelling, and itching have been reported but are generally mild and transient.
Studies of semaglutide and tirzepatide show that approximately 25% of weight loss may come from lean mass, including muscle (10). Retatrutide’s greater potency could potentially result in an even more pronounced loss of muscle, which may impair metabolic health and physical function.
In addition to the more common and normally mild-to-moderate gastrointestinal symptoms discussed earlier, GLP-1s have been linked to gastroparesis-like symptoms and other gastric issues. These include slow gastric emptying and small bowel motility, and gastric food retention (11). Gastroparesis itself is a disorder characterised by delayed gastric emptying due to impaired stomach muscle contractions and nerve function.
Slower stomach and bowel movement from GLP-1 drugs can leave food sitting in the stomach, which raises the risk of vomiting and aspiration during procedures, and makes symptoms such as nausea or reflux worse. In some cases, this buildup of undigested food can harden into a lump called a bezoar, which can cause pain or even block the stomach.
Retatrutide’s triple-agonist mechanism may produce similar or stronger effects on gastric motility.
GLP-1s can produce noticeable cosmetic changes due to rapid reductions in subcutaneous fat and metabolic stress. Loss of facial fat leads to hollowing of the cheeks and temples, sharper contours, and skin laxity, which is often described as ‘Ozempic face’ (17). A similar effect can occur in the body, with volume loss and loose skin in areas which naturally have low fat reserves (17). Retatrutide has the potential to accentuate these effects due to its ability to produce greater and more rapid fat loss.
Concerns have been raised about pancreatitis and pancreatic cancer with GLP-1–based drugs. However, studies to date have not shown a causal link. In Phase 2 trials of retatrutide, no cases of pancreatitis were detected. Some people had small increases in pancreatic enzymes, but these caused no symptoms and did not develop into pancreatitis (15). Interestingly, a study on mice found that low-dose retatrutide shrank pancreatic tumours to about one third their size, performing almost as well as a standard cancer treatment (16). Current evidence aside, we have no idea of the effects of long-term retatrutide use on pancreatic health and function.

The most significant concern surrounding retatrutide is the complete absence of long-term safety data. The longest treatment duration in published retatrutide studies is 68 weeks from the Phase 3 TRIUMPH-4 trial (15). For a medication intended for chronic use in obesity and diabetes, safety data over multiple years are essential. Long-term effects on bone density, muscle mass preservation, nutritional status, and organ function, including pancreas, gallbladder, heart, kidneys and liver, require investigation (15).
Phase 2 trials are not adequately powered to detect adverse events occurring at rates below approximately 1–2%. Hopefully, the Phase 3 programme, which involves thousands of participants, will help to identify less common safety signals (15).
There is currently limited information available regarding the effects of retatrutide in certain populations including:
We do not currently have human pregnancy safety data for retatrutide. Therefore, studies on its effects on fertility and foetal development are necessary before it can be used safely by women who may become pregnant. There is also no human research on whether retatrutide passes into breast milk or how it might affect a baby (15).
Retatrutide is broken down in a way that makes drug–drug interactions unlikely. However, because it slows gastric emptying, it may change how well some oral medicines are absorbed, especially those where even small changes in dose can increase the risk of an adverse reaction (15).
The long-term effects on weight and metabolic health after stopping retatrutide have not been studied. Evidence from similar GLP-1 therapies suggests that weight regain is likely once treatment ends, but the specific pattern and extent of this with retatrutide therapy remain unknown. There is also a lack of long-term evidence regarding the risk of nutritional deficiencies due to appetite suppression and the potential for metabolic adaptation, where the body compensates for weight loss by reducing energy expenditure (15).
Although understandably overshadowed by the potential physical issues, the use of retatrutide also raises social and psychological concerns. These include the risk of over-medicalising weight management (12) and encouraging cosmetic rather than medical use driven by social media pressures (13). Its appetite-suppressing effects may lead some people to become dependent on medication (14), while others may experience worsening body image or disordered eating (13). These trends can also increase stigma and social pressure on individuals who choose not to use such medications (12).

The release of any new, highly effective medication demands careful attention to be given to the ethical and practical challenges that determine how, when, and by whom it should be used. This raises a number of questions:
Q: Will its cost be so prohibitively expensive that it limits access for those people who need it most?
A: As obesity disproportionately affects lower-income populations, the people who need retatrutide most may struggle to access it.
Q: Will the supply chain be able to stand the demand?
A: Already we have seen semaglutide shortages and the problems that can bring. If retatrutide is as effective as preliminary results suggest, demand is likely to be considerable and perhaps exceed supply.
Q: Is there a risk of counterfeit or unregulated versions entering the market?
A: Although retatrutide is still in trials and not due for release for some time, it is already available on the black market. Medications from unregulated sources are associated with a number of risks including unknown ingredients, incorrect dosing, contamination, and the absence of any medical or legal protection.
Q: Might it encourage some people to not adhere to a healthy lifestyle?
A: There is a very real risk that some individuals may feel they no longer need to prioritise diet, physical activity, or other health behaviours if a medication appears to provide an easier alternative.
If retatrutide proves to be safe and effective, then current evidence suggests that suitable candidates for its use will include:
Retatrutide should not be used by anyone who does not meet the clinical criteria. Nor should it be used by people seeking cosmetic weight loss, unwilling to make lifestyle changes, expecting effortless results, or driven by trends or social pressure rather than medical need.
It is important to note that even when someone is deemed to be eligible to use retatrutide, they will need specialist supervision, with ongoing monitoring and support for nutrition, physical activity, and psychological wellbeing.
Current evidence suggests that retatrutide has the potential to radically transform obesity treatment. Not only can it produce unprecedented levels of weight loss, but also provide significant improvements in metabolic health. But we must approach it with both optimism and caution, as we have no data on the long-term effects of this novel treatment. Medical history is full of examples of promising medications and treatments that have been hailed as safe and effective only later to be shown to cause serious harm.
While retatrutide may ultimately prove valuable for people with severe obesity and metabolic disease, it does not negate the need for a healthy diet and lifestyle. Rather, it enhances it, as the maintenance of muscle mass will require regular participation in resistance training and an appropriate diet to support it.
Like all medications and treatments, the benefits of retatrutide must be weighed against the risks for each individual, and this should be decided by a qualified healthcare professional. It should not be viewed as a quick-fix replacement for a healthy lifestyle, but as a powerful treatment with potential risks, some as yet unknown, for the treatment of a serious medical condition and used only under medical supervision.
Retatrutide is not commercially available at the moment and has not been licensed for use outside of clinical trials. There are reports that it is being accessed by some on the black market to support weight loss, especially amongst the bodybuilding community. It is also available to buy online for ‘research purposes only.’ However, it is imperative to stress that these websites are completely unregulated and the safety and quality of their products is unknown. We would strongly advise using any medication like this unless it is licensed for the purpose it is being used and it is prescribed by an appropriately qualified healthcare professional.
To learn more about GLP-1 medications and their effects on appetite regulation, energy balance, and body composition, explore our GLP-1 and Weight Loss Medications course. It also covers how to apply this knowledge in practice, including exercise plans, client monitoring, and supporting long-term behaviour change through a holistic approach to weight management.
1) Jastreboff AM, Aronne LJ, Ahmad NN, Wharton S, Connery L, Alves B, et al. Retatrutide, a novel triple hormone receptor agonist, in adults with obesity: a phase 2 trial. N Engl J Med. 2023;389(25):2321 2334.
2) Eli Lilly and Company. Effect of retatrutide compared with semaglutide in adults with type 2 diabetes and inadequate glycaemic control with metformin with or without SGLT2 inhibitor (TRANSCEND T2D 2). ClinicalTrials.gov Identifier: NCT06260722. Updated 2026 Apr 13.
3) Eli Lilly and Company. A Study of Retatrutide (LY3437943) Compared to Tirzepatide (LY3298176) in Adults Who Have Obesity (TRIUMPH 5). ClinicalTrials.gov Identifier: NCT06662383. Updated 2026 Apr 13.
4) Eli Lilly and Company. A Study of Tirzepatide (LY3298176) in Participants With Obesity or Overweight With Weight Related Comorbidities (SURMOUNT 5). ClinicalTrials.gov Identifier: NCT05822830. Updated 2025 Nov 26.
5) FDA Labels & Safety Data (Semaglutide, Tirzepatide, Retatrutide). Accessed 2026. (Includes NEJM primary source links for STEP, SURPASS, and retatrutide Phase 2 trials.)
6) Zhou X, et al. Seven glucagon like peptide 1 receptor agonists and polyagonists for weight loss in patients with obesity or overweight: an updated systematic review and network meta analysis of randomized controlled trials. Metabolism. 2024;161:156038.
7) Rosenstock J, Frias J, Jastreboff AM, Du Y, Lou J, Gurbuz S, et al. Retatrutide, a GIP, GLP 1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double blind, placebo and active controlled, parallel group, phase 2 trial conducted in the USA. Lancet. 2023;402(10401):529 44.
8) Sanyal, A.J., Kaplan, L.M., Frias, J.P. et al. Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: a randomized phase 2a trial. Nat Med 30, 2037–2048 (2024). https://doi.org/10.1038/s41591-024-03018-2
9) Eli Lilly and Company. Retatrutide significantly reduces knee osteoarthritis pain and body weight in Phase 3 TRIUMPH 4 trial [press release]. Indianapolis (IN): Eli Lilly and Company; 2025–2026.
10) Wilding JPH, Batterham RL, Calanna S, Van Gaal LF, McGowan BM, Rosenstock J, et al. Impact of semaglutide on body composition in adults with overweight or obesity: exploratory analysis of the STEP 1 study. J Endocr Soc. 2021;5(Suppl 1):A16–A17.
11) Parkman HP, Rim DS, Anolik JR, Dadparvar S, Maurer AH. Glucagonlike Peptide 1 Receptor Agonists: The Good, the Bad, and the Ugly—Benefits for Glucose Control and Weight Loss with Side Effects of Delaying Gastric Emptying. J Nucl Med Technol. 2024;52(1):3 7. doi:10.2967/jnmt.123.266800.
12) Jensen SD, Gualano B, Andreassen P, Scagliusi FB, SturtzSreetharan C, Brewis A. Beyond the prescription: Global observations on the social implications of GLP 1 receptor agonists for weight loss. PLOS Glob Public Health. 2025;5(12):e0005516.
13) 13Medaris A. A new era of weight loss: Mental health effects of GLP 1 drugs. Monitor on Psychology. 2025 Jul–Aug;56(5):66.
14) Krug I, Dang AB, Portingale J, Li Y, Won YQ. Beyond Weight Loss: GLP 1 Usage and Appetite Regulation in the Context of Eating Disorders and Psychosocial Processes. Nutrients. 2025;17(23):3735.
15) Grodyńska B. The societal impact of GLP 1 receptor agonists. The Average Scientist. 2024 Nov 19.
16) Retatrutide Knowledge Base Editorial Team. Safety Profile of Retatrutide: Comprehensive Overview from Clinical Data. Retatrutide Knowledge Base; 2024 Oct 1. Updated 2026 Mar 18.
17) Marathe SJ, Bohm MS, Powell Z, Khan A, Pervaiz N, Wellen KE, et al. Retatrutide monotherapy matches the effectiveness of anti PD 1 immunotherapy in a preclinical model of pancreatic cancer. J Immunother Cancer. 2025;13(Suppl 2).
18) Rzany B, Griffiths CEM. Facial changes associated with GLP 1 receptor agonist–induced weight loss. J Eur Acad Dermatol Venereol. 2024;38(2):e125 e127.

Paul Orridge is a graduate in the field of sport, exercise and health, and has over 30 years’ experience within the fitness industry. In this time, he has performed a variety of roles including personal training, lecturing and writing. Paul now works as a freelance technical author and subject matter expert within the fitness industry. His work is based on his practical experience gained working with a diverse range of people from very unfit, overweight individuals to highly conditioned athletes, and is underpinned by the latest research.
And get the fast-paced world of personal training delivered straight to your inbox every week
Great news, you're on the list...